A Step for Peace: Middle East Nurses Uniting in Human Caring


This blog is about a small area of peace within a conflict zone. I’m referring to the cold war (sometimes erupting into hot-war violence) between Israel and the Palestinians. Dr. Jean Watson, world famous author and nurse theorist, has long observed that nurses of any nationality share similar values. They are all healers at heart. Observing that the Middle East is a region in dire need of healing, following the International Nursing Conference in Jerusalem in 2011, Jean visualized a conference as a forum for Palestinian and Israeli nurses to meet in a safe neutral setting, which is only possible in Jordan, as opposed to Israel or the Israeli-occupied Palestinian territories of the West Bank and Gaza. Susan and Jean reunited at this conference and subsequently, all of us have supported the event since the beginning.

This year’s conference in Aqaba, Jordan, (the eighth one, with previous conferences having been held in Jerusalem and Amman) was the largest ever, with approximately two hundred nurses. All presentations were simultaneously translated into the three language groups present: Hebrew, Arabic, and English. The atmosphere was sober in light of President Trump’s newly announced “deal of the century,” a proposal so strongly skewed toward Israel that it was immediately rejected by the Palestinians (who in any case were not consulted prior to its announcement). Everyone feels powerless to do anything to change the situation beyond simply deepening the professional cooperation and relationships between the Israeli and Palestinian nurses who frequently treat the same patients and seek to provide a continuum of care between the Israeli and Palestinian hospitals.

I learned that the United Nations has international policies stating that an occupying military power is responsible for providing healthcare to its occupied territories. Unfortunately, there is a large gap in the resources available for healthcare in the occupied territories as compared with Israel proper. This gap is evidenced by different life spans, infant mortality rates, and other common health measures. It reminds me of the gap between the health of blacks and whites in the era of American racial segregation, prior to the civil rights movement.
The conference featured research and case studies addressing issues arising in hospitals in Israel, the West Bank, and Gaza.
Below is an example of a case study which was completely new information to me: the establishment of “Human Milk Banks” to supply breast milk to new mothers who don’t produce enough milk on their own to sustain their newborns. Milk donors were traditionally called “wet nurses.” I learned that commercial powdered milk formula, made from cows’ milk, can be dangerous for neonates. The availability of human milk is thus essential. Studies have shown that mothers’ milk contains stem cells which become and remain part of the infant’s body for life.

Human milk banks are well established in the US and many European countries. But the Middle East poses special problems. In the absence of local human milk banks, mothers turn to their friends or acquaintances who might have milk to spare beyond their own babies needs. The problem here is that there is no guarantee that the milk is sterile, disease/infection-free, or otherwise safe. Orthodox Jewish women don’t want to accept milk from women who don’t strictly follow kosher dietary practices. But human milk banks combine anonymous donors’ milk from mothers whose milk is screened for good health and potential contamination, irrespective of the religion or race of the donors.
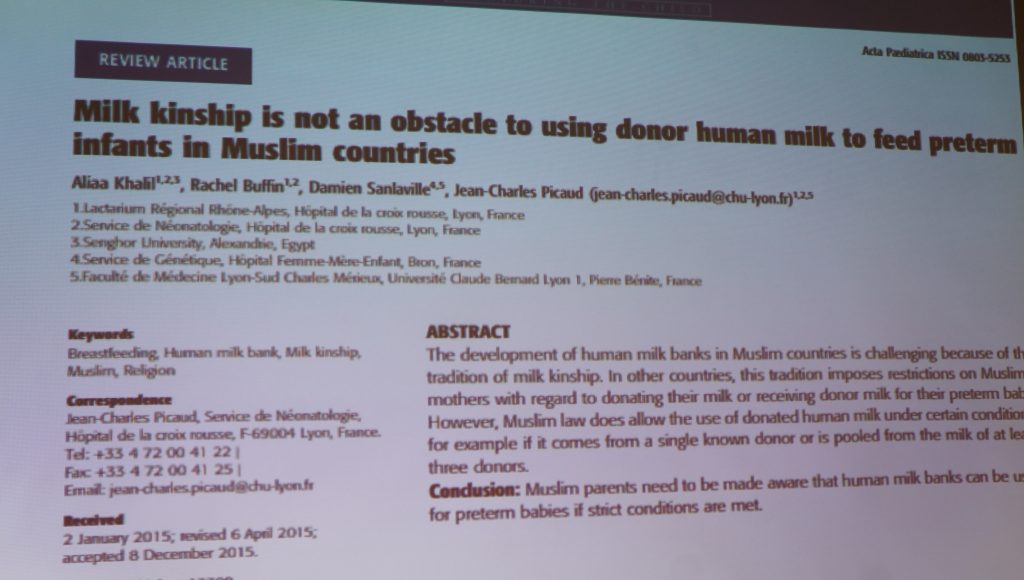
Moslems have a specific cultural belief called “milk kinship.” This is a traditional belief that for an unrelated male and female baby to share milk from the same woman, whether a mother or a wet nurse, creates a kinship that forbids future potential marriages by/among any babies who might share milk from the same woman. Thus this milk kinship tradition inhibits the establishment of milk banks in Moslem territories. I had no knowledge of this prior to this conference of the existence of this potential barrier to human milk banks that otherwise are essential to reducing infant mortality due to a mother not producing milk sufficient to sustain her baby.
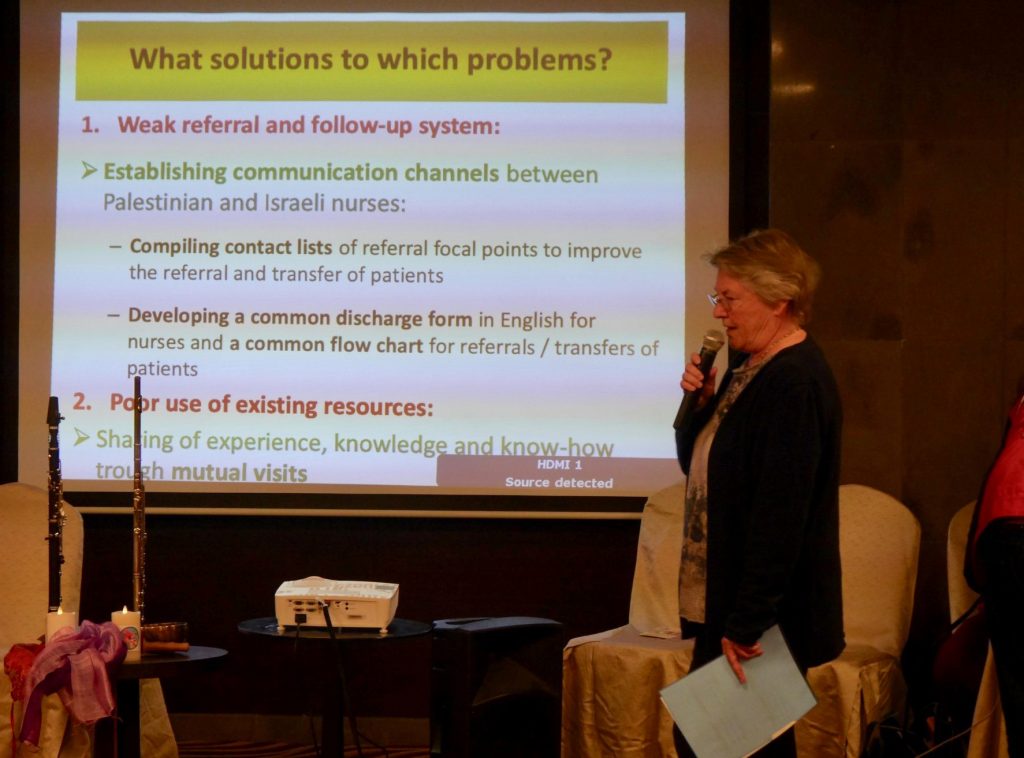
A larger and more generalized problem results from the Israeli military control and occupation of the Palestinian territories. There are many Israeli military checkpoints within the occupied Palestinian territories of the West Bank that create barriers to medical transfers. If an ambulance is transporting a Palestinian patient into Israel, that patient must be unloaded from the Palestinian ambulance and carried through the checkpoint to be put into an Israeli ambulance. The delays at border checkpoints can stretch for many hours. There are stories of babies being born in taxis waiting at the border, as well as patients dying because of delays in being transported to an Israeli hospital.
The situation in Gaza is even worse. A patient needing a medical treatment, such as chemotherapy or radiotherapy for cancer treatments, must apply for a permit to cross the border into Israel. Submitting applications and receiving the documents necessary for travel can take many weeks.
Only fifty percent of the permit applications submitted are ultimately granted. Being denied treatment through denying entrance to Israel is ultimately life-threatening. The import of any hardware or chemicals that might have a military application are forbidden by Israel, which unfortunately applies to chemotherapy agents as well as radiotherapy hardware.

Gazans suffer from a contaminated drinking water, which leads to widespread illness. Caused by limited access to fuel, electricity is available for only a few hours a day. The lack of fuel cripples their ability to treat the territory’s sewage. Thus thousands of gallons of untreated sewage flows into the Mediterranean every day. That sewage pollutes beaches in neighboring Israel and Egypt.
Unemployment in Gaza is the highest in the world: over 50{bf249dfdd09a1798812467d1b6a3ef7a33c47359bd28517191144d5320771815} for adult males and over 70{bf249dfdd09a1798812467d1b6a3ef7a33c47359bd28517191144d5320771815} for young males. Women are culturally inhibited from working many jobs, and thus female unemployment is even greater.
But the conference was not dominated exclusively by bad news. The opening presentation was led by a Jewish man and a Palestinian/Arab woman who have been working since 2003 to bring the art of clowning into Israeli and Palestinian hospitals. Since starting their work, they have created the Dream Doctors, currently an association of twenty-nine therapeutic clowns who practice their clown-magic in a hundred hospitals. They specialize in treating child-patients. Often the young patients that they treat ultimately succumb, which is a heart-breaking occurrence for any nurse-caregiver. They made the point that clowning is serious work. It is difficult to introduce fun and lightness into painful and traumatic medical environments. I was impressed with the depth of their work and their understanding of the challenges faced by nurses every day. I didn’t have the chance to ask them if they know American medical clown pioneer Patch Adams, but I assume that they must take inspiration from his work.


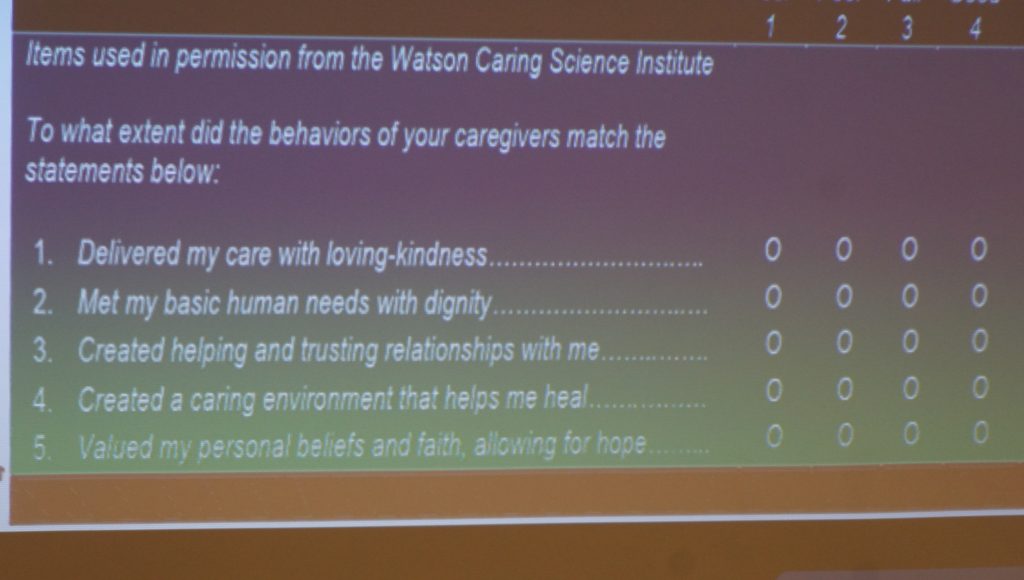
I like to call Dr. Jean Watson our twenty-first century Florence Nightingale. Her work has centered on helping nurses to get in touch with the original motivations that led them into the profession. A nurse can be loosely defined as anyone who is entrusted with the health of another. Professional nurses still have to fight for the respect that the profession deserves in light of the general orientation toward doctors, pharmaceuticals, and technology. As Florence Nightingale observed, the doctor can treat the patient, but it is the nurse who helps the patient to live by providing constant, consistent, and professional care. However, the first provision of Jean Watson’s processes for professional nurses is that they have to first take care of themselves, support their fellow nurses, and then finally be united in caring for their patients. I encourage readers to visit www.watsoncaringscience.org to learn more about Jean’s work. From her website, here are Jean’s ten “Caritas processes” to guide nurses in their professional practice:
- Sustaining humanistic-altruistic values by practice of loving-kindness, compassion and equanimity with self/others.
- Being authentically present, enabling faith/hope/belief system; honoring subjective inner, life-world of self/others.
- Being sensitive to self and others by cultivating own spiritual practices; beyond ego-self to transpersonal presence.
- Developing and sustaining loving, trusting-caring relationships.
- Allowing for expression of positive and negative feelings – authentically listening to another person’s story.
- Creatively problem-solving-‘solution-seeking’ through caring process; full use of self and artistry of caring-healing practices via use of all ways of knowing/being/doing/becoming.
- Engaging in transpersonal teaching and learning within context of caring relationship; staying within other’s frame of reference-shift toward coaching model for expanded health/wellness.
- Creating a healing environment at all levels; subtle environment for energetic authentic caring presence.
- Reverentially assisting with basic needs as sacred acts, touching mindbodyspirit of other; sustaining human dignity.
- Opening to spiritual, mystery, unknowns-allowing for miracles.


Below are some of the participants in this year's conference:















I played my one genuine Arabic song for my Palestinian friends.
0 Comments on A Step for Peace: Middle East Nurses Uniting in Human Caring
Join the Conversation